
Orthodontic Headgear and What It’s Used For
Orthodontic headgear—sometimes referred to as braces headgear—is a device used to correct severe bite problems. While braces can correct the position of your teeth, orthodontic headgear can help alter the alignment of your jaw by exerting tension on the braces via hooks, coils, elastic bands, and other attachable appliances. Orthodontic headgear can also be used to increase the space between teeth so that others can grow in. There are many different types of headgear used in dentistry, each of which can be configured to treat specific alignment disorders. They are most effective when used during early adolescence to the later teen years.
Purposes:
Orthodontic headgear is primarily used to correct bite alignment problems, referred to as anteroposterior discrepancies. The problem can involve the maxilla (upper jaw) and/or mandible (lower jaw). Issues include:
- Overjet, known commonly as “buck teeth,” in which the upper front teeth protrude at an outward angle toward the lip
- Overbite (retrognathism), in which the upper front teeth excessively overlap the lower front teeth
- Underbite (prognathism), in which the lower front teeth and jaw protrude in front of the upper front teeth
- Crossbite, in which the upper and lower teeth do not align when you bite down
The misalignment of the jaw and teeth is referred to as a malocclusion. An overjet and overbite are considered Class II malocclusions, while an underbite and crossbite are both Class III malocclusions. Some of these conditions can co-exist—such an overbite and crossbite—and require an individualized approach to correct both at once.
When an Overbite Can Become a Serious Problem :
Orthodontic headgear is generally used for children 9 and older with jaw growth discrepancies. At the stage in a child’s development, the bones of the jaw will still be actively growing. By holding back the growth of the jaw with consistent pressure, a malocclusion may be resolved noninvasively. This is often a far better solution than dealing with the problem as an adult when corrective surgery is more likely needed. By the age of 13 to 18, medical evaluation may be needed to determine if the child is still growing. This can be done with a cephalometric X-ray to inspect the bones of the spine (the clearest indicators of bone growth potential). If no further growth is expected, orthodontic headgear will offer little, if any, benefit. In non-growing children and adults, orthodontic headgear is occasionally used to correct severe spacing problems when braces alone are not enough.
How Headgear Works

As per its name, orthodontic headgear is worn on the head. There are different types used, some of which are attached with straps to the back of the head or neck and others of which are worn as a full-head cap.
A variety of appliances can be anchored to the headgear, including J-hooks, elastic bands, coil springs, retainers (to hold the teeth in place), power chains (to adjust the position of the teeth), lip bumpers, and facebows (external wire apparatus that extends across the face and into the mouth).
These appliances are attached to the braces with hooks. The orthodontist will then adjust the tension between the headgear and braces to stop, alter, or slow the growth of the jaw. The amount of pressure exerted is between 350 to 450 grams per side (more or less the same level of tension used for braces).
Broadly speaking, there are two types of headgear used for orthodontic treatment: a cervical and high- pull headgear or a reverse-pull facemask.
Cervical and High-Pull Headgear
Cervical and high-pull headgear are two headgear devices often used in tandem to treat Class II malocclusions. They can help correct overjet and overbite by holding the maxilla in place while allowing the mandible to grow out.
Cervical and high-pull headgear is comprised of three key components:
- Head cap: The head cap is held in place by a single strap behind the neck (cervical strap) and additional straps around the back of the head (high-pull straps).
- Facebow or J-hooks: A facebow is comprised of an outer bow that attaches to the headgear and an inner bow that attaches to the back teeth (molars). J-hooks are two separate wire apparatus, one end of which is attached to the headgear and the other of which hooks onto the braces.
- Attachment appliances: A variety of orthodontic bands, coils, and springs provide the tension needed to move the upper teeth and jaw backward.
Reverse-Pull Facemask
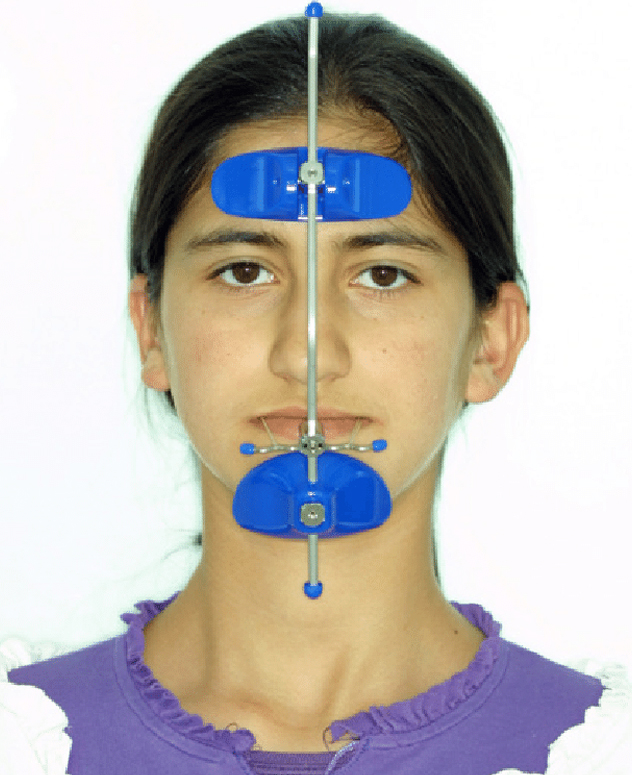
A reverse-pull facemask is an orthodontic device used to treat Class III malocclusions. They work by pulling the mandible forward so that it can catch up the growth of the maxilla.
The reverse-pull facemask is comprised of three key components:
- Face mask: The face mask consists of a forehead pad and chin cup that are connected to a fixed metal frame. The mask is held in place with either Velcro straps around the forehead or a stabilizing head cap.
- Mouth yoke: The face mask frame will have a horizontal mouth yoke onto which attachment appliances can be hooked.
- Attachment appliances: Elastics are typically used to connect the mouth yoke to your braces. By doing so, the maxilla is drawn forward without interfering with the alignment of the front teeth.
Newer devices include a palate expander that is fitted against the roof of your mouth like a retainer. Elastic bands are then attached to connection points on the expander and mouth yolk. The tension between the two is enough to hold the facemask in place without straps.
What to Expect
Whether you are being treated for an overbite or underbite, the orthodontic headgear will need to be worn for around 12 to 14 hours per day. Many orthodontists will advise you to wear the device at night, putting it on just after dinner and taking it off in the morning. Severe malocclusions may require up to 22 hours daily.
There will usually be a period of adjustment when first starting treatment, especially in young children. To adapt more comfortably, many orthodontists will recommend a ramping-up stage in which you wear the device for one hour on the first day and increase the duration by an hour every day until the target time is reached. As you begin to achieve results, your orthodontist will begin to adjust the tension on your headgear.
It is not unusual to feel discomfort after an adjustment, especially while chewing or talking. Tylenol (acetaminophen) or a nonsteroidal pain reliever like Advil (ibuprofen) or Aleve (naproxen) can usually help. Call your dentist if the pain is severe or persistent.
While you should remove the headgear whenever eating, you can use a straw for sipping fluids without having to remove the device each and every time. Your orthodontist will provide you with instructions and a journal to accurately log the number of hours you’ve worn the headgear each day.
Consistency is key to treatment success. If started at a younger age and used consistently, orthodontic headgear can correct some misalignment problems in as few as six months. On the other hand, every skipped day can set your progress back significantly and potentially undo all of the gains that you’ve made.